DCIS (Ductal Carcinoma in Situ)
The earliest form of breast cancer is known as DCIS (ductal carcinoma in situ). DCIS is also called stage 0 breast cancer.
DCIS is not invasive cancer and is not life-threatening. Having DCIS can increase the chance of developing invasive breast cancer. For this reason, a person with DCIS will require treatment, but not chemotherapy.
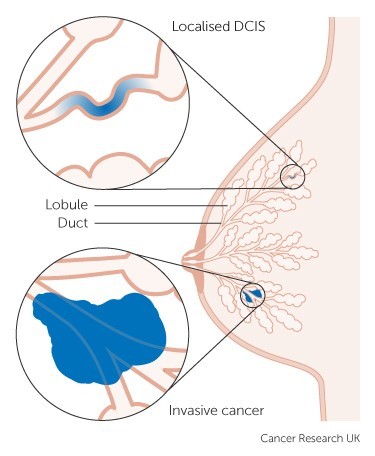
A diagnosis of DCIS means that cancer cells have formed inside the walls of the ducts, but haven’t invaded the surrounding tissue. Because they’re still confined within the duct walls, they can’t invade the blood or lymphatic vessels, which is how cancer usually spreads around the body. DCIS is sometimes called pre-invasive, non-invasive, or intraductal carcinoma.
Women can develop DCIS at any age, but it’s more common over age 50. Men can also get DCIS, but it’s rare.
Detecting DCIS
Prior to the introduction of breast screening, DCIS was usually detected after it had developed into a breast mass or produced nipple discharge. Now, it is commonly detected early in the form of micro-calcifications (tiny calcium deposits) seen on a mammogram, well before any mass can be felt. DCIS accounts for 22% of breast cancers detected in New Zealand’s free breast screening programme.
Breast calcifications occur commonly and most are benign, but some variations in size, shape and pattern can indicate that the micro-calcifications might be cancerous. If a mammogram shows that you have suspicious or indeterminate micro-calcifications, you will be referred to a specialist to complete the triple test – a clinical breast exam, imaging and a biopsy – to determine whether the calcifications are malignant or benign.
Classification of DCIS
Stage: All DCIS is classed as Stage 0 breast cancer as it is confined within the walls of the ducts.
Grade: This describes the appearance of cells viewed under a microscope, how much they differ from normal, healthy breast cells and how quickly they are growing and dividing.
- Low grade:
The cells still look quite similar to normal breast cells and are slow-growing. - Intermediate grade:
The cells look less like normal cells and are growing and dividing faster than normal. - High grade:
The cells look very different to normal cells and are growing and dividing rapidly. High grade DCIS has a higher risk of becoming invasive cancer within five years after diagnosis, and has a higher risk of recurring after treatment than low or intermediate grade.
Should DCIS be treated?
While DCIS itself is not life threatening, if left untreated it may eventually become an invasive cancer and spread into surrounding tissue. Not all cases behave this way, but currently it’s not possible to accurately predict which cases will not progress to invasive cancer and could be safely left untreated.
Large international clinical trials (e.g. the UK's LORIS trial and the LORD trial in the USA), aim to find out whether women over the age of 45 with low grade DCIS could be safely managed with active monitoring and no surgery.
Unfortunately, the results of these trials are many years away. Currently, it is common practice to surgically remove DCIS, in order to prevent patients developing invasive cancer.
Video
Webinar: Dealing with DCIS
Our webinar discusses what to expect when you have DCIS, from treatment options and follow-up to your risk of developing invasive breast cancer.
Treatment of DCIS
Surgery and radiation therapy
Most people with DCIS will be recommended surgery with radiation therapy unless mastectomy has been performed. The aim of surgery is to remove the abnormal cells and prevent the development of invasive cancer in the future.
Breast conserving surgery
If the involved area is small, breast conserving surgery could be recommended. Usually, no lymph nodes would need to be removed for examination during the surgery unless micro-invasion – a small amount of cancer cells spreading out of the ducts – is suspected.
Occasionally, a mammogram might underestimate the size of the affected area as not all DCIS forms calcifications. More than one surgical procedure might be needed to ensure all the cancer cells have been removed.
Following breast conservation surgery, whole breast radiation therapy is usually required to reduce the risk of recurrence; however in a select population with small volume, low risk disease this might sometimes be omitted.
Mastectomy
If the DCIS is spread over a large area or in several sections of the breast, then a mastectomy would likely be recommended.
A sentinel lymph node biopsy (SLNB) is usually performed in this situation to examine the first lymph node that drains the breast. This is because a mastectomy removes the lymph drainage pathways from the tumour so a SNLB can't be done later if invasive cancer is subsequently found in the surgical specimen.
Post-op radiation therapy isn’t needed due to the very low risk of recurrence when the breast has been removed.
Chemotherapy is not required for the treatment of DCIS as it does not spread beyond the breast.
Prognosis
Prognosis following treatment for DCIS is generally excellent, but there remains a very small risk that it may recur in the breast in the future, or that invasive cancer may develop. This risk is lower following mastectomy, but overall survival rates after DCIS treatment are the same for mastectomy as for partial mastectomy coupled with radiation therapy.
Because people with DCIS have ongoing close surveillance with regular mammograms, any local recurrence or new breast cancer is usually detected early and able to be successfully treated.
LCIS (Lobular Carcinoma in Situ)
LCIS (lobular carcinoma in situ or lobular neoplasia) is not actually breast cancer, but a marker of increased risk of developing breast cancer in the future. It can’t be felt or seen on breast imaging, and women with LCIS will not be aware of any symptoms. It’s usually detected as breast cell changes in biopsied tissue or in a surgical specimen.
LCIS differs from DCIS in that it is not considered a direct pre-cancerous change. If left untreated the affected tissue doesn’t progress to invasive cancer, but women with LCIS do have a higher risk of getting breast cancer; however, it is just as likely to occur elsewhere in the breast or in the opposite breast. Doctors usually recommend regular surveillance with breast checks and mammograms.
Treatment of LCIS
LCIS generally doesn’t need treatment unless there are other abnormal changes in the breast. The exception to this is a subtype known as pleomorphic LCIS, a variant with cells that look more abnormal and are growing more aggressively. If found on biopsy, surgical removal of the area is usually recommended.